The top 21 nutrition myths
With so many nutrition myths, it’s hard to know where to start. In this article we cover carbs, eggs, red meat, and a lot more. Each entry strikes at the heart of the debate and is followed by links to in-depth articles.

Last Updated:February 6, 2024
With all the information at our fingertips today, you’d think that nutrition myths would have become less pervasive than in our grandparents’ time.
Unfortunately, the internet is rife with misinformation, and it can be really difficult to tell what’s evidence-based without reading the original research yourself. Myths that were previously passed through word-of-mouth now spread like wildfire through social media, blogs, and even established media. Between a 24-hour news cycle, studies that are both long and difficult to read, and journalists scrambling for the latest viral hit, information often gets published without verification. And once we’ve assimilated a piece of information, we seldom think to challenge it — we treat it as fact.
As an educational organization that looks only at the evidence, we’ve taken the time to identify 21 nutrition myths that just won’t die. At the end of each section, you’ll find a link to pages that further explore the section’s topic with extensive references.
Myth 1: Protein is bad for you

Carbs and fats often take the blame for various health issues, but the third macronutrient isn’t always spared by the media. Protein has often been accused of harming bones and kidneys.
Let’s tackle those two claims one at a time.
Bone loss
More protein in the diet has been linked to more calcium in the urine. Two reasons have been suggested to explain this phenomenon:
- Your body draws from its calcium stores (in bones) to buffer the acid load caused by dietary protein. This has led researchers to suggest that higher protein intake could cause greater bone loss.[1]
- Most studies that looked at protein intake and calcium excretion list dairy products as a protein source,[2] so higher urinary calcium could simply be the result of higher calcium intake (i.e., more calcium in, more calcium out).
Therefore, looking only at calcium excretion wasn’t enough. Subsequent studies showed that dietary protein promotes dietary-calcium absorption[3] and that high protein intake “promotes bone growth and retards bone loss [whereas] low-protein diet is associated with higher risk of hip fractures.”[4]
What happens is that when you ingest more protein, you absorb more of the calcium in your food, so less calcium ends up in your feces. Later, your body gets rid of the calcium it doesn’t need, so more calcium ends up in your urine, but not as much as would have otherwise ended in your feces.[5] Therefore, an increase in protein intake leads to an overall decrease in calcium excretion, which points to an increase in calcium retention.
All in all, current evidence suggests that protein actually has a neutral or even protective effect on bones.[5][6]
Kidney damage
Other studies determined that high protein diets increased glomerular filtration rate (GFR), a marker for waste filtration in the kidneys.[7] It was argued that increased GFR was a sign that undue stress was put on the kidneys,[8] but later research has shown that kidney damage does not occur as a result of diets high in protein.[9][10]
In conclusion, randomized trials thus far have not shown that high-protein diets harm the bones or kidneys of otherwise healthy adults.[9]
The Truth: Protein, even in large amounts, isn’t harmful to your bones or kidneys (unless you suffer from a pre-existing condition).
Related articles:
Myth 2: Carbs are bad for you

For decades, fat was the enemy, but today, there’s a new scapegoat: carbs. Vilifying carbs and insulin seems to get more popular by the year.
Many people believe that the popular glycemic index and the lesser-known insulin index[11] rank foods by their “unhealthiness”. Yet the available research shows that low-glycemic diets, when compared to higher-glycemic diets, have either no effect or only modest beneficial effects on metabolic syndrome factors,[12][13][14][15][16][17][18] even in diabetics.[19][20][21] Furthermore, a low-glycemic diet doesn’t always lead to better glycemic control than do other diet patterns.[22]
Similarly, the carbohydrate-insulin model of obesity, which theorizes that obesity is caused by carbs and the insulin response they evoke,[23] is not well-supported by the evidence.[24][25]
In 2017, a meta-analysis of 32 controlled feeding studies was published.[26] Some of those studies were metabolic ward studies and some were free-living studies, but in each case, meals were supplied by the researchers, who wanted to ensure that each diet provided specific amounts of calories and nutrients (within each study, the diets were equal in calories and protein but not in fat and carbs).
So what were the results? Low-fat diets resulted in greater fat loss (by an average of 16 grams per day) and greater energy expenditure (by an average of 26 calories per day). This would give low-fat diets a fat-loss advantage, though one “so small as to be physiologically meaningless”.[26]
These results are consistent with those of long-term, free-living, randomized controlled trials designed to test a diet’s real-world effectiveness (meaning that the participants were given instructions but left to prepare their own meals). Meta-analyses show that keto, low-carb, and higher-carb diets lead to similar weight loss.[27][28]
Eating less carbohydrate (especially processed carbs) can be helpful if it helps you eat healthier. But if cutting carbs makes you eat worse or feel worse, or if you can’t stick with the diet, you should consider other options. If you wish to lose weight, what matters is not to replace fat by carbs or carbs by fat, but to end most days on a caloric deficit.
The Truth: As long as you do not overindulge, there is nothing inherently harmful about carbohydrates.
Related articles:
- High-carb, high satiety?
- Can one binge make you fat?
- Low-fat vs. low-carb? Major study concludes: it doesn’t matter for weight loss
- What should you eat for weight loss?
Myth 3: Fats are bad for you

Eat fat, gain fat, right? For many decades, the traditional way to lose weight has been to subject oneself to a low-fat diet, yet current evidence suggests that, given the same caloric deficit and protein intake, low-fat and low-carb diets produce similar weight losses.[17][26][29][27][28]
Moreover, while low-fat diets are not inherently unhealthy, shunning all fat from your diet can be dangerous because your body needs to consume at least some omega-3 and omega-6 fatty acids. As for saturated fat being a driver of cardiovascular disease — not necessarily a myth, but it's more complicated than most people think.
A high saturated fat diet can increase LDL-C, which increases the risk of cardiovascular disease.[30] However, saturated fatty acids are a heterogeneous group of fatty acids, and not all foods rich in saturated fat increase LDL-C (e.g., cheese, chocolate). Additionally, removing saturated fat from the diet doesn't always reduce the risk of CVD — it depends on what it's replaced with.
Basically, not all saturated fats are bad; they're only one piece of the puzzle; it's important to consider the overall dietary pattern.
At the end of the day, trans fat is the only kind of fat that has been shown to be categorically detrimental to health.[31] Naturally occurring trans fat and industrially produced trans fat seem to have a similar effect on blood lipids,[32] but you don’t need to worry about the minute amounts of trans fat naturally occurring in whole foods (notably dairy products).[33] The trans fat you need to shun is a byproduct of partially hydrogenated oils: this type of trans fat was once a common ingredient of processed foods — so common that trans fat consumption was linked to more than half a million coronary heart disease (CHD) deaths worldwide in 2010 alone.[34][35]
Partially hydrogenated fats, the predominant source of industrially produced trans fat, were banned in the US in 2015, and all products were supposed to be phased out by June 2018, but manufacturers received an extension until July 2019.[36]
The Truth: If you stay in a caloric surplus, a low-fat diet won’t make you lose weight. You need some omega-3 and omega-6 fatty acids, saturated fat won't necessarily give you a heart attack, and trans fat should be limited as much as possible.
Related article:
- Is saturated fat bad for your health?
- Does eating fat make you fat?
- Low-fat vs. low-carb? Major study concludes: it doesn’t matter for weight loss
- What should you eat for weight loss?
Myth 4: Egg yolks are bad for you
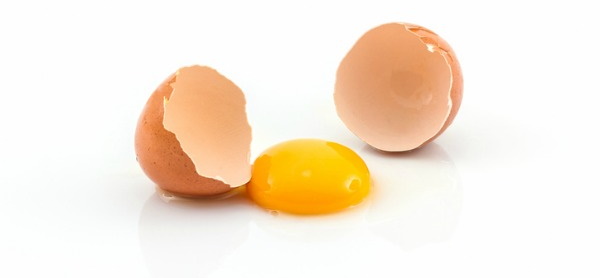
If there’s one thing the media is good at, it’s scaring you away from perfectly healthy foods.
Yes, foods high in cholesterol can increase LDL cholesterol in most people but to a fairly small extent on average.[37] Moreover, some of the micronutrients and other bioactive compounds in egg yolks could interfere with cholesterol absorption, and many studies have failed to find an increase in cholesterol in egg eaters.[38][39][40]
More to the point, although a review of cohort studies (a type of observational studies) associated higher consumption of cholesterol or eggs with higher risk of cardiovascular disease (CVD) and all-cause mortality in a dose-response manner,[41][42] clinical trials (a more rigorous type of study) found no association between eggs and CVD,[43][44][45][46][47][48] except in some people who “hyper-respond” to dietary cholesterol.[49][50]
The Truth: Eggs are a great source of protein, fats, and other nutrients. Their association with high cholesterol and cardiovascular disease has been severely overblown.
Related article:
Myth 5: Red meat is bad for you
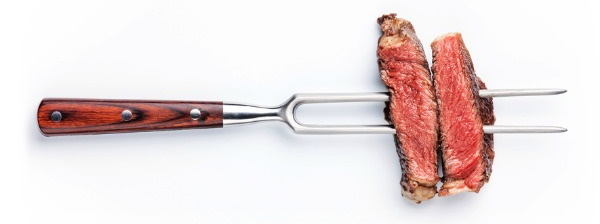
The common refrain: red meat causes cancer.
Absolute statements are why we have so many nutrition myths. Cancer is particularly difficult to discuss in absolutes. After all, almost everything we eat has the potential to be associated with cancer development,[51] yet red meat has been fingered as a likely culprit.
Some compounds — such as polyaromatic hydrocarbons (PAHs), found in smoked meats — have been found to damage the genome, and damaging the genome is the first step to potential cancer. Current evidence suggests that processed red meats, particularly those that are more charred during cooking, can pose a greater cancer risk for people with poor diets and lifestyles.[52][53]
But if you moderate your red meat intake, exercise regularly, eat your fruits and veggies, consume adequate fiber, don’t smoke, and drink only in moderation, red meat’s effect on cancer isn’t something to worry too much about.
There is some evidence that eating a lot of red meat or processed meat might increase the risk of type 2 diabetes and of various other cardiometabolic diseases, but that evidence is of lower quality. Still, if you want to be especially cautious, you can limit your intake to three servings per week (1 serving of beef = 3 oz = 85 grams).
The Truth: Fears about red meat causing cancer are overly broad. The types of red meat that have strong associations with cancer center around regular intake of cured, smoked, or highly processed meat. Making healthy lifestyle choices (such as eating a balanced diet rich in whole foods, staying at a healthy weight, exercising, and not smoking) is more important overall than micromanaging your intake of red meat.
Related articles:
- Scientists found that red meat causes cancer ... or did they?
- Does red meat cause cancer?
- Headline whiplash: Red meat is good for you now?
- How can I make red meat healthier?
- Is halving red and processed meat intake heart healthy? (for ERD subscribers)
Myth 6: Salt is bad for you

Some myths contain a grain of truth. Studies have associated excess salt with hypertension (high blood pressure),[54] kidney damage,[55] and an increased risk of cognitive decline.[56][57]
However, salt (sodium) is an essential mineral; its consumption is critical to your health. The problem occurs when you consume too much sodium and too little potassium.
Another issue is the source of all that salt. The average North American eats an incredible amount of salty processed foods[58] — which means that people who consume a lot of salt tend to consume a lot of foods that are generally unhealthy. That makes it hard to tease apart sodium’s effects from overall dietary effects. Except for individuals with salt-sensitive hypertension,[59] the evidence in support of low sodium intakes is less conclusive than most people imagine.[60][61] As it stands, both very high and very low intakes are associated with cardiovascular disease.[62]
The Truth: Salt reduction is important for people with salt-sensitive hypertension, and excessive salt intake is associated with harm. But a drastic decrease in salt intake has not shown uniform benefit in clinical trials. Most people will benefit more from a diet of mostly unprocessed foods than from micromanaging their salt intake.
Myth 7: Bread is bad for you

Bread has taken a beating over the past few years (especially white bread). The bread detractors generally make two arguments against its consumption:
- Bread will make you fat.
- Bread contains lots of gluten, which is bad for you.
Bread will not inherently make you fat, but it tends to be dense in calories and is therefore easy to overeat. And of course, most people eat bread with other high-calorie foods, such as butter, peanut butter, jam, or honey. This can lead to a caloric surplus and thus to weight gain over time. Moreover, while bread can be part of a healthful diet, a bread-centric diet can crowd out more nutrient-rich foods, notably fruits and vegetables.
Also, some people choose to avoid bread entirely because of its gluten content. Gluten critics claim that any amount of gluten (a protein, ironically, and not a carb) is a danger to all. While “all” is an exaggeration, it is indeed possible to suffer from non-celiac gluten sensitivity.[63][64] However, it is also possible for your wheat sensitivity[65] to be caused by other compounds, such as FODMAPS (short-chain carbohydrates known to promote intestinal distress by fermenting and producing gas),[66][67] which are present in wheat, yes, but also in many other foods, such as legumes, apples, and milk (and other dairy products containing lactose).
White bread vs. whole-wheat bread
You may have heard that eating bread is all right as long as it’s whole-wheat bread. While white bread (made from wheat flour) and whole-wheat bread provide a similar number of calories, whole-wheat bread has a lower glycemic index and insulin index, and so its consumption results in a lower insulin release. For that reason, and because of its higher fiber and micronutrient content, whole-wheat bread is claimed to be healthier than white bread.
What the media frequently fails to mention is that the actual differences between white bread and whole-wheat bread are relatively small. Yes, whole-wheat bread has a higher fiber content — but this content pales compared to that of many fruits and vegetables. You most definitely don’t have to eat whole-wheat products to get enough fiber in your diet! And yes, white bread does lose more micronutrients during processing — but those micronutrients are often reintroduced later (the bread is then called “enriched”).
The Truth: Although some people are sensitive to wheat, the gluten content isn’t necessarily to blame, and other foods may also be implicated. Bread (or any other food) will not inherently cause weight gain unless its consumption puts you in a caloric surplus. Whole-wheat bread is claimed to be far healthier than white bread, but they aren’t that different, and neither contains high levels of fiber or micronutrients.
Related articles:
- Gluten-intolerant? There’s a pill for that
- Does gluten make you fat?
- Can autism be helped by gluten-free, casein-free diets?
- Can cutting out FODMAPs cut out IBS symptoms?
Myth 8: HFCS is far worse than sugar

High fructose corn syrup (HFCS) is a blend of glucose and fructose commonly used to sweeten food products.
Early evidence led to the belief that fructose could cause fatty-liver disease, as well as insulin resistance and obesity. By extension, HFCS is frequently said to be unhealthy because it is high in fructose.
The reality is that there isn’t always more fructose in HFCS than in sugar. Liquid HFCS has a fructose content of 42–55%. Sucrose, also known as table sugar, is 50% fructose. The difference (−8% to +5%) is too slight to matter.
The Truth: HFCS and table sugar are very similar from a health perspective. Although HFCS may sometimes contain more fructose, the difference is negligible.
Related article:
- What is the difference between high fructose corn syrup and sugar?
- Is high fructose corn syrup worse than sugar?
Myth 9: Dietary supplements are necessary

This is a favored line of thinking among supplement companies and health gurus. One argument is that crops are becoming poorer in nutrients[68] due to intensive agriculture and increasing levels of carbon dioxide (CO2) in the atmosphere.[69] Another argument is that foods contain a mess of unknown compounds, in addition to known “poisons” such as the dreaded saturated fat, cholesterol, gluten, and FODMAPs.
No wonder that more than one-third of Americans take a multivitamin/mineral. Better cover one’s bases, or so the thinking goes. Alas, there is no evidence that taking a multi will increase your life expectancy. While it may support your health in some ways, by ensuring adequate intakes of underconsumed nutrients, it could hurt it in others, by making you overconsume some nutrients to the point where they may harm your health.
Fact is, multis are seldom well formulated. Due to cost and space considerations (people willing to take one pill a day may balk at taking ten), multis are often rich in micronutrients abundant in a healthy diet and poor in others you are more likely to need. Try to focus on what you actually need by tweaking your diet and, in special cases, by supplementing with specific micronutrients — such as vitamin B12 if you are vegan or a senior, or vitamin D if your bare skin seldom gets enough sun exposure.
In fact, many foods you’ll find at the supermarket are already fortified with the micronutrients you’re most likely to lack. Milk, for instance, is frequently fortified with vitamin D, whereas salt is iodized, and enough foods are fortified with folic acid that you’re as likely to get too much as not enough.
In that light, it may be tempting to take the next step and live on meal replacements, with all the necessary nutrients added in and none of the aforementioned “poisons”. That could work — if we actually knew the optimal intakes for all nutrients.
We learn a little more each day, but there’s still much we don’t understand about food components and their interactions with different systems in our bodies, especially because those interactions can differ between individuals. So, until we reach a perfect understanding of the human body and its nutritional needs, you’re safer eating a varied diet of little-processed foods than ingesting the same meal replacement day after day after day. And it’ll taste better.
The Truth: Supplements have their uses. Some people may benefit from supplementing specific vitamins or minerals. But supplements should complete a healthy diet — not replace it.
Related articles:
Myth 10: Food nutrients > supplemental nutrients
How often have you heard the claim that natural, whole foods are always better than synthetic supplements? In general, the word “natural” has a positive connotation, whereas “synthetic” or “chemical” has a negative one.
The truth, of course, isn’t so clear-cut. Some compounds are more effective in supplemental form. One example is the curcumin in turmeric. On its own, your body cannot absorb it well, but taken in liposomal form[70] or supplemented with piperine, a black pepper extract, the bioavailability of curcumin increases dramatically.
The same goes for vitamins. For instance, phylloquinone (K1) is tightly bound to membranes in plants and thus is more bioavailable in supplemental form.[71] Likewise, folic acid (supplemental B9) is more bioavailable than folate (B9 naturally present in foods), although that may not always be a good thing.
The Truth: With regard notably to vitamins, foods are not always superior to supplements.
Myth 11: Fresh is more nutritious

Fresh produce has a natural appeal to many people. “Fresh” just sounds better than “canned” or “frozen”, doesn’t it? But just because a food is fresh doesn’t necessarily mean it’s more nutritious.
Fresh produce is defined as anything that is “postharvest ripened” (if it ripens during transport) or “vine-ripened” (if it is picked and sold ripe, at a farmer’s fresh market or at a farmer’s roadside fruit stand, for instance).
Frozen produce is generally vine ripened before undergoing minimal processing prior to freezing. Most vegetables and some fruits are blanched in hot water for a few minutes prior to freezing to inactivate enzymes that may cause unfavorable changes in color, flavor, smell, and nutritional value.[72] While there are some differences between fresh and frozen for select nutrients in select fruits and vegetables, overall, the nutritional content is very similar.[73]
Canned produce is usually vine ripened, like frozen produce, but it tends to undergo a lot more processing, several forms of which can break down some essential nutrients, such as nitrates,[74] almost entirely. However, one should remember that cooking is also a form of processing, and that different ways of cooking can affect the produce’s nutrient content and bioavailability[75] more than its being fresh, frozen, or canned. An additional issue with canned produce, however, is that salt and sugar are often added as preservatives to vegetables and fruits respectively — so look at the label.
The Truth: There’s little difference between fresh and frozen produce, nutrient-wise. Canned produce tends to undergo a lot more processing, but remember that cooking is a form of processing too. Overall, fresh and frozen produce might be more nutritious than canned produce, but eating enough whole-food fruits and vegetables is more important than how they were processed.
Related article:
Myth 12: Foods labeled “natural” are healthier

It is natural to think that foods labelled “natural”, “all natural”, or “100% natural” are healthier, but what do those labels actually mean?
The answer isn’t as simple as it should be. To begin with, we need to divide foods into two categories. In the first category, we have meat, and in the second, everything else.
Meat
In the United States, the US Department of Agriculture (USDA) must approve label claims for meat, including the “natural”, “no hormones” and “no antibiotics” claims. However, what the “natural” claim means is just that the product is no more than “minimally processed” and does not contain any artificial ingredients (including chemical preservatives and artificial flavoring or coloring). It doesn’t necessarily mean that the cow wasn’t given antibiotics and hormones before it became a food product (such as milk or meat, though the USDA only concerns itself with the latter).
Now, if hormones or antibiotics were given to a cow, they might be found in its meat, which would then contain artificial ingredients. But is the meat actually tested, or can it be labelled “natural” simply if nothing was added to it? (Which is to say, if nothing was added to the meat after the cow was killed and thus became beef.)
Considering that (1) the “no hormones” and “no antibiotics” claims require special documentation and (2) the “natural” claim only covers product processing and ingredient addition, the answer seems to be that a piece of beef can be labelled “natural” even if the originating cow was given hormones or antibiotics.
Other foods
For foods other than meat, the Food and Drug Administration (FDA) steps in. At present, however, the FDA does not have a formal definition for the “natural” label. (This may soon change though, as this label is currently undergoing a review process to determine if it should be better defined.)
Meanwhile, the FDA considers “natural” any food to which nothing artificial or synthetic was added “that would not normally be expected to be there / in that food”. Yes, that’s awfully vague. A little more precisely, the FDA states that a product without colorants (regardless of source) or synthetic substances (including artificial flavoring) can be labelled “natural”.
Note that, for the FDA, the label “natural” doesn’t reflect “food processing or manufacturing methods” or “food production methods, such as the use of genetic engineering or other forms of genetic modification, the use of pesticides, or the use of specific animal husbandry practices”.
The Truth: Overall, the “natural” label isn’t tightly regulated. Importantly, neither the USDA nor the FDA defines “natural” in relation to the healthfulness of the food. In other words, a “natural” label doesn’t guarantee the product is healthful (though it might be).
Myth 13: You should eat “clean”

This statement is not so much a myth as a jumble of misconceptions. First of all, people seldom agree on what “eating clean” actually means. For some, it means shunning specific foods for religious or ethical reasons (animal products, for instance). For others, it means eating only fresh, raw, natural, organic foods. For others still, it means making sure that their fruits and veggies are free of pesticides. One common point of clean diets is their focus on exclusion: they tell you what clean eating is by telling you what not to eat.
Only plant-based food
Veganism can be considered a prime example of a clean diet, as it shuns all animal products both for ethical reasons and for better health. But although vegans and vegetarians do tend to be healthier on average,[76] this may be due to reasons unrelated to food. For instance, people who stick to a vegetarian diet are more likely to also stick to an exercise regimen and neither drink in excess nor smoke.[77][78]
As it stands, compared to people eating a varied omnivorous diet, vegans (and, to a lesser extent, vegetarians) are more likely to get suboptimal amounts of some nutrients, such as L-carnitine or vitamin B12. However, those nutrients can easily be supplemented — nowadays, there are even plant-based options for EPA, DHA, and vitamin D3.
Only raw food
Some “clean eating” gurus recommend that you only eat your food raw, so as not to “denature” its nutrients. As an absolute, this rule is a myth. Raw milk can contain harmful bacteria. Raw eggs contain avidin, a protein that can bind biotin and thus lead to biotin deficiency if consumed frequently,[79][80] and you’ll digest more protein from cooked than raw eggs.[81][82] Cooking can reduce the nitrate content of vegetables (bad) but also their oxalate content (good). You can’t generalize.
Only organic food
“Organic is better.” This statement is presented as self-evident, on the principle that “natural” is good, whereas “synthetic” is bad. So far, however, the few studies that have investigated the effect of organic food on clinical health outcomes have failed to consistently link organic foods (from plants or animals) to better health.[83][84]
It doesn’t mean that organic foods and better health are definitely not linked, but the issue is complex, and in some cases, you’ll be trading one health risk for another. For instance, a 2018 test of protein powders revealed that the organic ones had about half the amount of BPA (an industrial chemical) but twice the amount of heavy metals.
One misconception is that no synthetic substance can be used to grow organic crops, whereas the National List of Allowed and Prohibited Substances makes some exceptions. Another misconception is that no pesticide can be used to grow organic crops. But while organic produce (notably fruit) less often has synthetic pesticide residue than conventional produce,[85] natural (organic) pesticides exist, are used to grow organic crops, and are not always better for the consumer or the environment.[86]
Only pesticide-free produce
Pesticide residues in food are a valid concern, though it should be noted that the Pesticide Data Program (PDP) of the United States Department of Agriculture (USDA) has consistently found that the vast majority of the food on the market contains either no detectable residues or residues below the tolerable limits set by the Environmental Protection Agency (EPA).
When found, pesticide residues were similarly low in organic and conventional produce, but there is some evidence that even very low doses of pesticides might still elicit physiological effects.[87] These effects, whether beneficial, neutral, or harmful and from organic or conventional pesticides, are not well studied.
So what is a consumer to do? The practical solution is quite simple: rinsing, peeling when possible, and cooking can reduce the amount of pesticide left on your produce,[88][89] whether this produce is organic or not.
The Truth: “Clean eating” is tough to define, as gurus don’t even agree on which foods are clean and which are not. Stick to the basics. Favor whole foods (but don’t feel like any small amount of processed foods will kill you), eat organic if you wish to and can afford it, and peel or wash all your vegetables and fruits.
Related article:
Myth 14: You should “detox” regularly

“Detox diets” are the ultimate manifestation of the “clean eating” obsession. Such diets commonly limit foods to plant-based juices, sometimes seasoned with a supplement. After a few days of that regimen, you’re supposed to be cleansed of …
Well, detox-diet companies don’t really know. A 2009 investigation of ten companies found they couldn’t name a single “toxin” eliminated by any of their fifteen products — let alone prove that their products worked. Strictly speaking, toxins are plant- or animal-based substances poisonous to humans. However, for many detox gurus, “toxins” also include heavy metals … and everything synthetic, not just toxicants (man-made poisons, such as pollutants or pesticides), but also preservatives, high-fructose corn syrup (HFCS), etc.
Alas, even when a substance really is noxious, a “detox diet” won’t help. Acute toxicity is likely to be a medical emergency, whereas chronic toxicity can be handled better by a well-fed body — not one weakened by a severely hypocaloric diet. Your liver, kidneys, lungs, and other organs work around the clock to remove harmful substances and excrete the waste products of metabolism. By reducing your intake of the nutrients that those organs need to perform these functions, a detox diet can hinder your body’s natural detoxification process! If you wish to promote this process, your best bet is to load up with various foods that can help your organs to work optimally,[90] such as cruciferous and other fibrous veggies.[90][91]
Detox diets are not necessarily safe, either. Every now and then a case report emerges about potential risks, such as kidney damage from green smoothies[92] or liver failure from detox teas.[93]
But if detox diets are more likely to harm than help, what explains their current popularity? One answer is quick weight loss. Deprive your body of carbs and you can exhaust its glycogen stores in as little as 24 hours. The resulting loss of several pounds can convince you that the diet had a positive effect.[94] When the diet ends and you resume your regular eating habits, however, the glycogen and associated water come rushing back in, and with them the pounds you’d shed.
So when people feel better from a detox diet, is it just a placebo effect? Not always. People on a detox diet might eat fewer calories yet more fruits and vegetables and thus more micronutrients. They may also stop consuming foods that don’t agree with them (in other words, detox diets work as de facto elimination diets).
The Truth: Focus on sustainable health habits, such as eating nutritious foods. Ample protein, leafy greens, and foods chock-full of vitamins and minerals are not just tastier than anything a “detox diet” has to offer, they’re also way better for you (and your liver detoxification pathways, ironically). A detox diet might make you feel better, but that’s usually because of the increased whole-food intake, not because any form of detoxification is taking place.
Related articles:
Myth 15: Eating often will boost your metabolism
It’s easy to trace this myth back to its origin. Digestion does raise your metabolism a little, so many people believe that eating less food more often keeps your metabolism elevated.
However, the size of the meal matters, too: fewer but larger meals means fewer but larger spikes in metabolism. Moreover, some studies suggest that having smaller meals more often makes it harder to feel full, potentially leading to increased food intake.[95]
More to the point, the evidence shows that, given an equal amount of daily calories, the number of meals makes no difference in fat loss.[96]
The Truth: Digestion does slightly increase your metabolic rate, but the frequency of your meals will have less effect on your weight than their total caloric content at the end of the day.
Related article:
Myth 16: You shouldn’t skip breakfast
“Breakfast is the most important meal of the day” is something we have all heard before from parents, doctors, health bloggers, and ad campaigns. But the health perks of consuming a regular breakfast have been overhyped.
People on #TeamBreakfast mention observational studies showing that, on average, breakfast skippers have a higher BMI.[97] However, clinical trials have shown that personal preference is a critical factor. Some people will subconsciously compensate for all the calories they skipped at breakfast, while others won’t feel cravings of the same magnitude. In one trial, women who didn’t habitually eat breakfast were made to consume it, and they gained nearly 2 pounds over four weeks.[98] Individual responses do vary, so don’t try to force yourself into an eating pattern that doesn’t sit well with you or that you can’t sustain — it may end up backfiring.
Another popular claim is that skipping breakfast can crash your metabolism. But studies in both lean and overweight individuals have shown that skipping breakfast does not inherently slow your resting metabolic rate (RMR).[99][100]
However, the “don’t skip breakfast” mantra might hold true for people with impaired glucose regulation.[101]
The Truth: You don’t need to eat breakfast to be healthy or lose weight. You should base your breakfast consumption on your preferences and personal goals. Feel free to experiment to see if you want to make skipping breakfast a habit.
Related article:
Myth 17: To lose fat, don’t eat before bed

Some studies show a fat-loss advantage in early eaters, others in late eaters. Overall, early eaters seem to have a slight advantage — nothing impressive.[102][103] Trials, however, imperfectly reflect real life. In real life, there are two main reasons why eating at night might hinder fat loss, and both are linked to an increase in your daily caloric intake.
The first reason is the simplest: if, instead of going directly to bed, we first indulge in a snack, then the calories from that snack are calories we might have done without.
The second reason is that, when we get tired, we tend to eat to keep going, with a predilection for snack foods or tasty treats. So if we stay awake at night — especially to work or study, but even just to watch TV — we’re more likely to eat, not out of hunger, but to help fight sleepiness.
The Truth: Eating late won’t make you gain weight, unless it drives you to eat more. Resisting tasty, high-calorie snacks can also be harder after a long day.
Related article:
Myth 18: To lose fat, do cardio on an empty stomach

Let’s get one thing out of the way. If you exercise near maximal capacity (HIIT, sprints, heavy lifting, etc.), you should eat one or two hours before, or you’re likely to underperform. Most people who choose to exercise on an empty stomach, however, opt for some moderate form of cardio (aerobic exercise), such as jogging, and in that case, performance and energy expenditure are about the same in the fed state and the fasted state.
If you exercise in the fasted state, you’ll burn more body fat, of course, but that won’t make it easier for you to use body fat as fuel during the rest of the day (when you’re fed). You’ll also burn a tiny bit more muscle, but you’ll grow it back faster afterward too — it seems to balance out, as long as you get enough protein after your workout and over the whole day. Finally, cardio suppresses appetite less in the fasted state than in the fed state, but that doesn’t translate into a significant difference in daily caloric intake.
People with impaired glucose regulation may wish to avoid exercising on an empty stomach, and might want to avoid skipping breakfast even when they don’t exercise.[101]
The Truth: There’s very little difference between cardio in the fed or fasted state with regard to fat loss, muscle preservation, daily caloric intake, or metabolic rate. Therefore, what really matters is you. Some people feel lighter and energized when they do cardio on an empty stomach, while others feel light-headed and sluggish. Fed or fasted state: pick whichever makes you feel better.
Related article:
Myth 19: You need protein right after your workout

When you exercise, you damage your muscles, which your body then needs to repair, often making them more resilient (bigger) in the process. The raw material for this repair is the protein you ingest, and yes, after exercising, your muscles are more sensitive to the anabolic effect of protein, thus creating a (still controversial[104][105]) window of opportunity — the “anabolic window”.
“You need protein right after your workout” may not be a myth so much as an exaggeration. What matters most is your daily protein intake, but ideally, you’ll want a postworkout dose of protein in the range of your desirable minimum protein intake per meal (0.24–0.60 grams per kilogram of body weight, so 0.11–0.27 g/lb). If you’ve been exercising on an empty stomach, you’ll be in a negative protein balance, so take this dose as soon as possible. Otherwise, try to take it within the next couple of hours — the exact size of your “anabolic window” depends on how much protein you’re still digesting.
The Truth: Unless you’ve been exercising on an empty stomach, you don’t need protein immediately after your workout, but you might benefit from 0.24–0.60 grams per kilogram of body weight (0.11–0.27 g/lb) within the next couple of hours. What matters most, however, is how much protein you get over the course of the day.
Related articles:
- A second look at protein quantity after exercise
- How much protein do you need per day?
- Protein Intake Calculator
Myth 20: Creatine will increase your testosterone but cause hair loss and kidney damage

No, unlikely, and no. As one of the most widely used supplements, creatine has been subjected to a whole host of spurious claims. Let’s tackle these three common ones.
Testosterone increase
Creatine helps you exercise harder by making it easier for your cells to regenerate adenosine triphosphate (ATP), a source of energy. To this day, there is no strong evidence that creatine can raise testosterone levels.
Three randomized controlled trials (RCTs), totalling 60 male participants, reported small yet statistically significant increases in either testosterone or dihydrotestosterone (DHT) from doses ranging from 5 to 25 grams of supplemental creatine.[106][107][108] However, ten other RCTs, with a total of 218 male participants, reported no effect on testosterone from doses ranging from 3 to 25 grams of supplemental creatine.[109][110][111][106][112][113][114][115][116][117][118][110]
People wishing to optimize their testosterone levels should focus on better-proven options. Suboptimal levels of sleep, exercise, calories, vitamin D, magnesium, and zinc can decrease testosterone production.
Hair loss
The idea that creatine might increase hair loss stems from a single RCT in which the participants (20 healthy young male rugby players) saw a small but statistically significant increase in DHT after supplementing with creatine for 21 days.[106] When DHT, a potent metabolite of testosterone, binds to DHT receptors on the hair follicles of the scalp, those follicles may shrink and stop producing hair.[119][120]
To date, this RCT is the only one to have tested creatine’s effect on DHT. However, twelve others have tested creatine’s effect on testosterone: two reported a small increase,[107][108] but ten reported no effect.[109][110][111][106][112][113][114][115][116][117] Of those twelve RCTs, five also tested creatine’s effect on free testosterone, the form that gets converted into DHT, and all reported no effect (no statistically significant increase or decrease was detected).[109][112][114][110][116]
Now, creatine could nonsignificantly increase free testosterone yet significantly increase DHT because a small percent increase in free testosterone, which can convert into DHT, could lead to a much greater percent increase in total DHT. So it’s technically possible that creatine might have some effect on hair loss — but current evidence and mechanistic data indicate it’s quite unlikely.
Kidney damage
Blood levels of creatinine (a byproduct of energy production) are used as an indicator of kidney function, but elevated levels caused by supplemental creatine are not a sign that your kidneys underperform.[121][122]
No adverse effects on kidney function were found in …
- People with healthy kidneys taking up to 10 grams of creatine per day. Short- and long-term trials are numerous and the results are consistent.[123][124][125][126][127][128][129][130]
- People with healthy kidneys taking more than 10 grams of creatine per day. Long-term trials are few, however, so caution is warranted.[130]
- People with suboptimal kidney function taking up to 5 grams of creatine per day. Trials in this population are scarce, so caution is warranted.[131][132][133][134]
If you plan to have your creatinine levels tested, stop taking creatine at least 3 weeks before the test to avoid a false positive.
The Truth: Out of all the supplements out there, creatine is one of the most extensively researched. The vast majority of the evidence indicates that this supplement is safe for long-term use and is unlikely to harm your kidneys, cause hair loss, or increase your testosterone.
Related articles:
- Can creatine increase your testosterone levels?
- Does creatine cause hair loss?
- Is creatine safe for your kidneys?
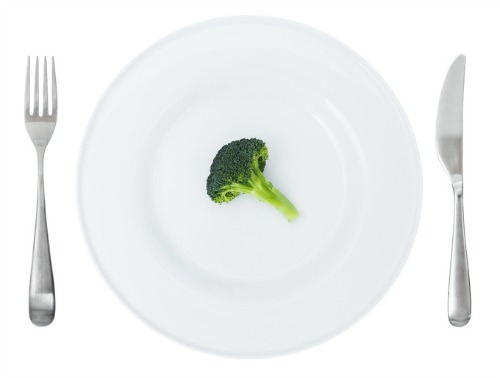
Myth 21: Negative calorie foods are the key to weight loss

‘Negative calorie’ foods are the holy grail for weight loss — foods that have fewer calories than your body uses to digest them. Imagine the weight loss you could achieve if you consumed a food that created a caloric deficit after you ingested it. Amazing!
Sadly, these types of foods likely don't exist. Even celery, often cited as the ultimate negative calorie food, provides a small 2.24 kcal per 100 grams consumed. Yet foods that are typically thought of as ‘negative calorie’ often possess some beneficial traits, such as being low in total calories and high in fiber and water content.
These foods (celery, tomatoes, lettuce, etc.) are likely to be more filling, which could result in you eating less. So, their regular consumption may aid in weight loss.
The Truth: There is no evidence that a food can possess negative calories, thereby directly contributing to weight loss. But foods typically categorized as ‘negative calorie’ items tend to be high in water and fiber, so their consumption may lead to weight loss because you consume less food overall.
Related articles:
Misinformation in the mainstream media
You’ve likely heard most of these 21 myths repeated at one time or another — by a friend, on a blog, or somewhere in the media. Misinformation is rampant and difficult to identify, and unfortunately spreads much faster than facts.
And really, this is just the tip of the iceberg. You’ll often see sensationalist headlines based on a study with unsurprising results. In mid-2017, for instance, the media went into a frenzy of similar headlines claiming that a review paper[135] showed that coconut oil was “bad” for you; of course, when we analyzed the studies, we found that coconut oil, like most other natural foods, has both benefits and downsides. Even the major, eight-million dollar study led by Christopher Gardner of Stanford University, which compared the weight-loss effects of low-fat and low-carb diets,[17] was misrepresented all over the media. (According to Dr. Gardner, Examine.com did the very best job in covering the study.)
That’s why we have an entire team poring over the research. And not just one or two studies, either — but the entire body of evidence.
Want more evidence-based information?
This is what we do. We analyze research, make sense of it, and give it context. We’re an educational organization that prides itself on avoiding clickbait or sensationalist headlines.
Because we all want to be healthy, it’s easy to fall for nutrition myths, fad diets, or the latest miracle supplement. That’s why we created the Examine Membership — the easiest way for you to stay up to date on the latest nutrition and supplement information, save time and money, and improve your health.