
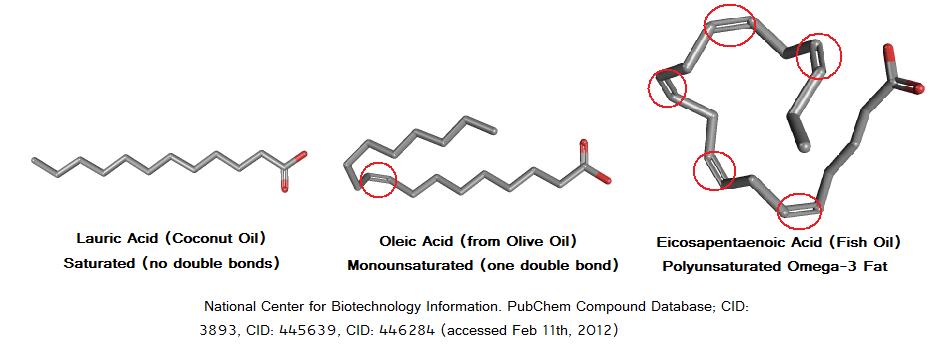
The fat you eat (and the fat you store in your body) is made up of different types of fatty acids, each with a long chain of carbon atoms bonded together. Saturated fatty acids (SFAs) have no double bonds, whereas monounsaturated fatty acids (MUFAs) have one and polyunsaturated fatty acids (PUFAs) have two or more. The “kinks” those bonds form in fatty acid chains prevent the fatty acids from packing close together, which is why unsaturated fats are liquid at room temperature, whereas saturated fats usually aren’t (they’re packed solid).
Saturated fats are fatty acids with no double bonds, which is why they are usually solid at room temperature.
However, classifying fatty acids by degree of saturation does not predict how they are handled by the body.[1] Based on the length of its tail (the number of carbons in its chain), a saturated fat belongs to one of four main subcategories, each with its own biological effects.

Even within each subcategory, the various fatty acids have different health effects.
For example, although palmitic acid and stearic acid are both long-chain saturated fats, the former causes a greater increase in blood cholesterol levels.[2] Similarly, although caprylic acid and capric acid are both medium-chain saturated fats, the former results in a larger blood ketone response.[3]
Those variations greatly limit our ability to discuss saturated fat in general. Just as it would be inappropriate to generalize the effects of poisonous mushrooms to all mushrooms, it is inappropriate to generalize the effects of one kind of saturated fat to all kinds of saturated fat.
Saturated fats differ by their length (as indicated by the number of carbons in the fatty acid chain) and can each have unique biological effects.
Medium-chain triglycerides, aka MCTs
Medium-chain triglycerides (MCTs) are saturated fats containing 6–10 carbons. Long-chain triglycerides (LCTs) are saturated fats containing 12–18 carbons.
The ketogenic nature of MCTs has led to a growing interest in their use as a food supplement. Traditionally, they’ve served to mimic a ketogenic diet (a very restrictive, very-low-carbohydrate diet) in children with epilepsy.[4] Today, MCTs are also advertised as helping with fat loss, exercise performance, and brain health, though the evidence is limited.
The richest natural source of MCTs, coconut oil, is ≈14% MCTs by weight,[5] so you’d need to eat 100 grams of fat (900 kcal) from coconut oil to consume 14 grams (1 tablespoon) of MCTs. For that reason, people interested in MCTs usually turn to concentrated MCT oils.
Medium-chain triglycerides (MCTs) and long-chain triglycerides (LCTs) are two groups of saturated fats. Your body metabolizes MCTs and LCTs very differently. Unlike LCTs, MCTs are not easily obtained in large quantities from whole foods (the best source is coconut oil, but you would need to eat 7 tablespoons to obtain 1 tablespoonful of MCTs), so they won’t be considered throughout this article.
Why do people think saturated fat is so unhealthy?
A quick history lesson on why people think saturated fat is unhealthy.
Since the 1950s, many studies have linked the consumption of saturated fat with increases in blood cholesterol levels.[6] Those studies, combined with observational research on the association between diet and heart disease,[7] led Dr. Ancel Keys to propose the diet-heart hypothesis, which suggests that saturated fat raises blood cholesterol levels and thus increases the risk of heart disease.[8][9]

Despite some researchers arguing that there were significant flaws in the data Keys used to support his claims,[10] the diet-heart hypothesis persisted and resulted in the belief that a heart-healthy diet should limit saturated fat. Within the academic and medical communities, this conclusion was widely accepted as fact, and it influences official dietary guidelines even today.
Research conducted throughout the later half of the 1900s led Dr. Ancel Keys to propose the diet-heart hypothesis, which posits that dietary saturated fat raises blood cholesterol levels and thus increases the risk of heart disease.
Saturated fat and your heart
Since the diet-heart hypothesis led to official recommendations against saturated-fat intake, it makes sense to address heart disease first.
How does arterial plaque form?
Our arteries are lined with a layer of cells called the endothelium, which functions as a selectively permeable barrier between our blood and the rest of our body. This is akin to our intestinal tract, which allows for the absorption of some nutrients but not others. In our blood, one of the “nutrients” that penetrates the endothelium is low-density lipoprotein (LDL), whose primary job is to transport cholesterol throughout the body.
The key event for the formation of plaques in arteries is the retention of LDL particles in the space beneath the endothelium (called the intima).[11] Once there, LDL is more susceptible to becoming oxidized, which signals the immune system to attack because oxidized LDL is seen as harmful to the body. This inflammatory response involves certain white blood cells called macrophages that literally “eat” the oxidized LDL particles. The LDL-engulfing process turns macrophages into foam cells, which can’t function properly and accumulate into the fatty build-up we call plaque.

As you can see, several events need to occur for heart disease to develop. This helps explain why heart disease has numerous environmental and genetic risk factors such as diabetes, obesity, smoking, lack of exercise, and infection.[12]
Any process that affects LDL retention and oxidation or inflammation is going to influence plaque formation and the risk of suffering from heart disease. Therefore, it makes sense to look at how saturated fat affects each of these processes.
Heart disease is most commonly the result of atherosclerosis (the buildup of plaque in arteries). Atherosclerosis happens when LDL particles penetrate arterial walls, become oxidized, and are attacked by white blood cells.
Effects of saturated fat on blood lipids
Saturated fat’s effects on blood lipids were thoroughly investigated in a systematic review and meta-analysis published by the World Health Organization (WHO) in 2016.[13] This meta-analysis included 84 randomized controlled trials (RCTs) involving a total of 2,353 healthy adults; it evaluated the effects of replacing 1% of caloric intake from carbohydrates or unsaturated fats with 1% of caloric intake from saturated fat.
To be included in the analysis, all studies were required to meet stringent criteria, so as to best isolate the effects of dietary substitution. For example, all food was provided to the participants, calories and protein were matched between diets, and all interventions lasted at least two weeks. The results are summarized in the table below.

Eating saturated fat instead of unsaturated fat or carbohydrates consistently increased lipid and lipoprotein concentrations in the blood. The one exception was a reduction in triglycerides when saturated fat was consumed instead of carbohydrates. Importantly, these effects were found to be consistent between sexes and across a wide range of baseline blood-lipid values and saturated-fat intakes (1.6–24.4% of calories). They were also consistent between studies, whatever the year of publication.
An important limitation of this meta-analysis is that it could not differentiate between the various food sources of the nutrients, which is an important consideration we shall discuss later. Moreover, studies investigating hydrogenated oils, fish oils, and medium-chain triglycerides were excluded.
Saturated fat increases lipid and lipoprotein concentrations in the blood when compared to carbohydrates, monounsaturated fat, and polyunsaturated fat.
LDL and HDL
Compared to carbohydrates and unsaturated fats, saturated fat raises the levels of lipoproteins and most blood lipids. These changes have well-researched implications for the risk of developing heart disease.
The greater the number of LDL particles in the blood (LDL-P), the more likely some will pass into artery walls, become oxidized, and kickstart plaque formation.[11] Therefore, to predict heart disease, LDL-P matters more than LDL-C,[14][15] which is simply a measure of the amount of cholesterol being carried by LDL particles.
If two people have the same LDL-C but one has cholesterol-rich LDL (large, “fluffy” particles) and the other cholesterol-poor LDL (smaller, denser particles), the second will have a greater LDL-P (more LDL particles total) and be at greater risk of heart disease.
The WHO meta-analysis didn’t cover LDL-P.[13] However, it did report the levels of apolipoprotein B (apoB), the protein component of LDL. Since each LDL particle has one molecule of apoB, apoB concentrations provide a good estimate of LDL-P concentrations and are a strong predictor of heart disease risk.[16][17]
To predict heart disease, LDL-P (the number of LDL particles) matters more than LDL-C (the amount of cholesterol those particles carry). There is one molecule of apolipoprotein B (apoB) in each LDL particle, so apoB is a good estimate of LDL-P. Consuming saturated fat (instead of unsaturated fat) increases apoB concentrations — and therefore your heart-disease risk.
High-density lipoprotein (HDL) removes cholesterol from arteries and plaques, protects the endothelium from damage, and inhibits LDL oxidation.[18]
HDL basically does the opposite of LDL. While calling HDL-C “good cholesterol” and LDL-C “bad cholesterol” is simplistic, studies do show that a higher ratio of LDL-C to HDL-C (and of total cholesterol to HDL-C) leads to a higher risk of heart disease. Those ratios matter more than your absolute numbers for LDL-C, HDL-C, and even total cholesterol.[19]
The WHO meta-analysis reported that eating more saturated fat increased HDL-C, but the increase was one-tenth that of LDL-C. Therefore, the ratio of LDL-C to HDL-C (and of total cholesterol to HDL-C) increased,[13] and with it the risk of heart disease.
A similar pattern was seen with apoA1, the major protein component of HDL particles, akin to apoB for LDL particles. Although replacing unsaturated fat by saturated fat led to increases in apoA1, the increase was only 30–60% that in apoB.[13] The ratio of apoB to apoA1 is considered a better predictor of heart-disease risk than other blood lipid biomarkers and their ratios.[20][21] If apoB increases more than apoA1, then the apoB-to-apoA1 ratio increases, and with it the risk of heart disease.
The HDL-C and apoA1 numbers reflect the amount of HDL in the blood. HDL has cardioprotective effects, but while eating saturated fat (instead of unsaturated fat) increases both HDL-C and apoA1, it increases LDL-C and apoB even more.
Finally, the triglyceride to HDL-C ratio represents a strong, independent predictor of heart disease when LDL-C levels are below 160 mg/dL,[22] and has similar predictive ability as LDL-C for determining the extent of atherosclerosis in at-risk patients.[23] Having a triglyceride-to-HDL-C ratio above 3.8 is associated with having more small, dense LDL particles, which are especially susceptible to oxidation.[24]
The WHO meta-analysis reported that eating more polyunsaturated fat reduced the ratio, whereas eating more carbohydrates increased it, when saturated-fat intake was reduced.[13] However, the changes were very small and not of clinical significance. A 10% reduction in calories from saturated fat would increase the triglyceride-to-HDL-C ratio by a mere 0.16 if more carbohydrates were eaten, and decrease it by only 0.04 if more polyunsaturated fat were eaten.
The triglyceride-to-HDL-C ratio correlates with the number of small, dense LDL particles and represents a strong risk factor for heart disease. However, changes in saturated-fat intake have little effect on this ratio.
Effects of saturated fat on inflammation
Plaque development requires that the immune system attack oxidized LDL particles within the arteries. Therefore, reducing systemic inflammation could help fight atherosclerosis, and in this manner decrease the risk of heart disease.[25][26]
Saturated fat may worsen systemic inflammation by increasing the absorption of lipopolysaccharides (LPS),[27] which are bacterial endotoxins that strongly stimulate our immune system.[28][29] Even very small serum concentrations of LPS, on a picogram scale, have the potential to elicit in humans an inflammatory response with a clear dose-response relationship.[30]
However, a systematic review found no consistent associations between consumption of saturated fat and a variety of inflammatory biomarkers, including cytokines, adipokines, acute-phase reactants, and cell adhesion molecules.[31] Clearly, the role of saturated fat on inflammation is not straightforward.
Still, one RCT reported that, compared to a diet high in SFAs, a diet high in MUFAs decreased LDL oxidation, a diet high in omega-6 (n-6) PUFAs increased it, and a diet high in omega-3 (n-3) PUFAs did not affect it.[32] The study authors attributed those differences to the fatty-acid composition of the LDL particles (i.e., to whether they contained mostly SFAs, MUFAs, or either kind of PUFAs).
Saturated fat may raise endotoxin levels to a greater extent than unsaturated fat, but it does not appear to affect systemic inflammation. Omega-6 polyunsaturated fat appears to increase LDL oxidation more than saturated fat (which is bad), whereas monounsaturated fat significantly reduces it (which is good).
Effects of saturated fat on heart disease
Up to this point, we have reviewed the effects of saturated fat on heart-disease risk factors rather than on heart disease itself.
The step between the two should be a small one, but that’s where things turn weird: despite a logical theoretical framework connecting diets high in saturated fat to atherosclerosis, meta-analyses of observational studies haven't reported consistently strong associations between saturated fat intake and risk of coronary heart disease, stroke, or cardiovascular disease in general.[33][34]
Even long-term RTCs that assessed hard endpoints of heart disease (such as suffering a heart attack, or dying from one) reported inconsistent links with saturated-fat intake. For instance, one meta-analysis reported that every 5% reduction in calories from SFAs (replaced by PUFAs) reduced the risk of heart disease by ≈10%,[35] but another reported that replacing SFAs by PUFAs was protective only when the PUFAs included both n-3 and n-6 fatty acids — replacing SFAs by only n-6 PUFAs tended to increase the risk of heart disease.[36]
One reason for the discrepancies is the failure of many studies to isolate the effects of altering saturated-fat intake. For example, some studies gave dietary advice to only one of the intervention groups — advice such as eating more plant-based foods; eating more n-3 PUFAs from fish and seafood; eating less sugar; and eating less trans-fat from margarines, shortenings, and partially hydrogenated oils.[37] When looking only at trials that minimized confounding factors, we see that replacing SFAs with primarily n-6 PUFAs has no effect on the risk of developing heart disease or dying from it.[37]
Neither observational studies nor RCTs support the notion that eating a diet high in saturated fat strongly increases the risk of developing heart disease or dying from it.
Understanding the difference between heart-disease risk factors and actual rates of heart disease
So, what gives? We have evidence that eating more saturated fat (instead of unsaturated fat) increases known risk factors for heart disease, such as blood lipids, but studies looking at the big picture do not find a link between saturated fat and heart disease. How can this be?
The simple answer is that fat intake is but a single piece of the heart-disease puzzle. Eating more saturated fat may increase your risk of developing heart disease, but that doesn’t mean you will develop heart disease. Conversely, banning all saturated fat from your diet does not make your heart attack proof.
In other words, rather than singling out any food or nutrient, we need to consider a person’s overall diet and lifestyle.
Let us use dairy as an example.
Dairy fat is ≈70% saturated fat,[38] making it a prime target for nutritional interventions. However, results from observational and experimental studies on the effects of dairy products on blood lipid levels are not conclusive,[39][40] and can even appear contradictory. For instance, there is RCT evidence that diets high in saturated fat from butter increase LDL-C, but that diets equally high in saturated fat from cheese might not.[39] Different dairy products, such as butter and cheese, have different food matrices (structures in which the food compounds are arranged), and thus different metabolic effects.[41]
Similarly, one meta-analysis reported a lack of significant associations between heart disease mortality and high intakes of meat or dairy products (including milk and cheese). [42] However, high intakes of processed meat did increase the risk of heart disease. It is well established that processed meats contain several carcinogenic compounds, which can influence heart disease risk.[43]
Whether saturated fat is good or bad for your heart may depend on what it is replacing — or being replaced by — in your diet. For example, replacing saturated fat by carbohydrates from whole grains is associated with a reduced risk of heart disease, whereas replacing saturated fat by carbohydrates from refined grains fails to confer the same benefit.[44] Similarly, replacing SFAs by plant-based MUFAs is associated with a reduced risk of heart disease, whereas replacing SFAs by animal-based MUFAs is not.[45]
If you care about your heart, you can’t just focus on saturated fat — or on any other nutrient. You need to look at the foods that provide it, and beyond that, at your overall diet and lifestyle. Doing otherwise means missing the forest for the trees.
Saturated fat and your brain
Studies in animal models and test tubes generally support the position that, compared to diets high in MUFAs or n-3 PUFAs, diets high in SFAs (and, to a lesser extent, diets high in n-6 PUFAs) have detrimental effects on brain development and cognitive function.[46][47] However, whether results in animals can be applied to humans is questionable.
Unfortunately, human studies are scarce. One study reported that eating a diet high in SFAs (from palm oil) increased self-reported anger (4.7 vs. 2.2 out of 5 points) and overall mood disturbances (13 vs. 7 out of 20 points) compared to eating a diet high in MUFAs (from hazelnut oil).[48] Other studies have reported that eating SFAs alters brain activation during cognitive tests and at rest, although the implications of these findings are not known.[49][50]
Studies in animals suggest that diets high in saturated fat may impair cognitive function and brain development. However, studies in humans are few and inconclusive.
Saturated fat and your weight
Appetite
Weight gain or loss depends greatly on caloric intake. According to a review of 24 studies, different types of fat affect subjective appetite similarly, at least in the short-term (e.g., single-meal assessments), in spite of satiety hormones being affected more by saturated than unsaturated fat.[51] However, differences in study protocols and participants make it difficult to draw overarching conclusions.
The effects of fat type on appetite regulation are not clear, but compared to monounsaturated and polyunsaturated fats, saturated fat appears to be either equally filling or slightly less filling.
Thermogenesis
Compared to meals high in unsaturated fat, meals high in saturated fat tend to result in lower levels of post-meal energy expenditure and fatty-acid oxidation.[52] Studies using isotope tracers indicate that the body would rather use unsaturated than saturated fats as an energy source.[53][54] However, long-term studies are inconsistent.[52]
Compared to unsaturated fat, saturated fat reduces energy expenditure and fat oxidation, but the long-term implications are not clear.
Activity
Eating more monounsaturated fat in place of saturated fat appears to spontaneously increase physical activity levels.[48]
Compared to unsaturated fat, saturated fat might reduce energy expenditure via reductions in physical activity.
Saturated fat and your hormones
Testosterone
Several RCTs have been conducted to evaluate the effects of dietary fat (amount and type) on men’s testosterone levels. To best understand these studies, we must first briefly discuss what they measured.
- Tightly bound testosterone. About two-thirds of the testosterone in your blood is bound to sex-hormone-binding globulin (SHBG). Your body can’t use it.
- Loosely bound testosterone. About a third of the testosterone in your blood is bound to albumin. Your body can use it, with some effort.
- Free testosterone. A small percentage of the testosterone in your blood (1–4%, as a rule) just floats around freely. Your body can readily use it.
Together, your loosely bound testosterone and your free testosterone compose your bioavailable testosterone, which has a greater impact on your health than your total testosterone.
Two studies with large sample sizes, controlled diets, and direct measurement of free testosterone reported that, compared to high-fat diets (33–40% of calories), low-fat diets (14–19% of calories) reduced total testosterone levels in healthy men, but did not alter levels of free or bioavailable testosterone.[55][56] Two other studies with smaller sample sizes, less accurate measurement methods, and less dietary control reported reductions in both total and free testosterone levels.[57][58]
Compared to diets high in fat (30–40% of calories), diets low in fat (14–19% of calories) appear to reduce total testosterone levels, but not necessarily free testosterone levels. In all cases, the reductions are fairly small and not clinically significant.
The big picture
Compared to monounsaturated fat (MUFAs) and omega-6 polyunsaturated fat (n-6 PUFAs), saturated fat (SFAs) does increase several risk factors for heart disease. However, compared to n-6 PUFAs only, SFAs also reduce some risk factors. In other words, eating more MUFAs appears to have the most favorable effect on risk factors for heart disease overall, whereas SFAs and n-6 PUFAs are on relatively equal footing.
There is some evidence that, compared to monounsaturated fat, saturated fat might have a negative effect on cognition, appetite, and energy expenditure; but further research is required.
A diet low in fat (14–19% of calories) might reduce total testosterone levels by 10–15% in otherwise healthy men. Total testosterone remains within normal range, however, and the biologically active free testosterone appears unaffected. Clinical significance is not known.
References
- ^Poudyal H, Brown LShould the pharmacological actions of dietary fatty acids in cardiometabolic disorders be classified based on biological or chemical function?Prog Lipid Res.(2015 Jul)
- ^Grundy SMInfluence of stearic acid on cholesterol metabolism relative to other long-chain fatty acidsAm J Clin Nutr.(1994 Dec)
- ^Vandenberghe C, St-Pierre V, Pierotti T, Fortier M, Castellano C, Cunnane STricaprylin alone increases plasma ketone response more than coconut oil or other medium chain triglycerides: an acute crossover study in healthy adultsCurr Dev Nutr.(2017 Mar)
- ^Neal EG, Chaffe H, Schwartz RH, Lawson MS, Edwards N, Fitzsimmons G, Whitney A, Cross JHA randomized trial of classical and medium-chain triglyceride ketogenic diets in the treatment of childhood epilepsyEpilepsia.(2009 May)
- ^Orsavova J, Misurcova L, Ambrozova JV, Vicha R, Mlcek JFatty Acids Composition of Vegetable Oils and Its Contribution to Dietary Energy Intake and Dependence of Cardiovascular Mortality on Dietary Intake of Fatty AcidsInt J Mol Sci.(2015 Jun 5)
- ^KEYS A, ANDERSON JT, GRANDE FPrediction of serum-cholesterol responses of man to changes in fats in the dietLancet.(1957 Nov 16)
- ^KEYS A, GRANDE FRole of dietary fat in human nutrition. III. Diet and the epidemiology of coronary heart diseaseAm J Public Health Nations Health.(1957 Dec)
- ^Keys A, Menotti A, Aravanis C, Blackburn H, Djordevic BS, Buzina R, Dontas AS, Fidanza F, Karvonen MJ, Kimura NThe seven countries study: 2,289 deaths in 15 yearsPrev Med.(1984 Mar)
- ^Keys A, Menotti A, Karvonen MJ, Aravanis C, Blackburn H, Buzina R, Djordjevic BS, Dontas AS, Fidanza F, Keys MHThe diet and 15-year death rate in the seven countries studyAm J Epidemiol.(1986 Dec)
- ^Reiser RSaturated fat in the diet and serum cholesterol concentration: a critical examination of the literatureAm J Clin Nutr.(1973 May)
- ^Tabas I, Williams KJ, Borén JSubendothelial lipoprotein retention as the initiating process in atherosclerosis: update and therapeutic implicationsCirculation.(2007 Oct 16)
- ^Lusis AJAtherosclerosisNature.(2000 Sep 14)
- ^World Health OrganizationEffects of saturated fatty acids on serum lipids and lipoproteins: a systematic review and regression analysis(2016)
- ^Allaire J, Vors C, Couture P, Lamarche BLDL particle number and size and cardiovascular risk: anything new under the sun?Curr Opin Lipidol.(2017 Jun)
- ^Otvos JD, Mora S, Shalaurova I, Greenland P, Mackey RH, Goff DC JrClinical implications of discordance between low-density lipoprotein cholesterol and particle numberJ Clin Lipidol.(2011 Mar-Apr)
- ^Contois JH, McConnell JP, Sethi AA, Csako G, Devaraj S, Hoefner DM, Warnick GR, AACC Lipoproteins and Vascular Diseases Division Working Group on Best PracticesApolipoprotein B and cardiovascular disease risk: position statement from the AACC Lipoproteins and Vascular Diseases Division Working Group on Best PracticesClin Chem.(2009 Mar)
- ^Sniderman AD, Williams K, Contois JH, Monroe HM, McQueen MJ, de Graaf J, Furberg CDA meta-analysis of low-density lipoprotein cholesterol, non-high-density lipoprotein cholesterol, and apolipoprotein B as markers of cardiovascular riskCirc Cardiovasc Qual Outcomes.(2011 May)
- ^Feig JE, Feig JL, Dangas GDThe role of HDL in plaque stabilization and regression: basic mechanisms and clinical implicationsCoron Artery Dis.(2016 Nov)
- ^Millán J, Pintó X, Muñoz A, Zúñiga M, Rubiés-Prat J, Pallardo LF, Masana L, Mangas A, Hernández-Mijares A, González-Santos P, Ascaso JF, Pedro-Botet JLipoprotein ratios: Physiological significance and clinical usefulness in cardiovascular preventionVasc Health Risk Manag.(2009)
- ^McQueen MJ, Hawken S, Wang X, Ounpuu S, Sniderman A, Probstfield J, Steyn K, Sanderson JE, Hasani M, Volkova E, Kazmi K, Yusuf S, INTERHEART study investigatorsLipids, lipoproteins, and apolipoproteins as risk markers of myocardial infarction in 52 countries (the INTERHEART study): a case-control studyLancet.(2008 Jul 19)
- ^Walldius G, Jungner I, Aastveit AH, Holme I, Furberg CD, Sniderman ADThe apoB/apoA-I ratio is better than the cholesterol ratios to estimate the balance between plasma proatherogenic and antiatherogenic lipoproteins and to predict coronary riskClin Chem Lab Med.(2004)
- ^da Luz PL, Cesena FH, Favarato D, Cerqueira ESComparison of serum lipid values in patients with coronary artery disease at 70 years of ageAm J Cardiol.(2005 Dec 15)
- ^da Luz PL, Favarato D, Faria-Neto JR Jr, Lemos P, Chagas ACHigh ratio of triglycerides to HDL-cholesterol predicts extensive coronary diseaseClinics (Sao Paulo).(2008 Aug)
- ^Hanak V, Munoz J, Teague J, Stanley A Jr, Bittner VAccuracy of the triglyceride to high-density lipoprotein cholesterol ratio for prediction of the low-density lipoprotein phenotype BAm J Cardiol.(2004 Jul 15)
- ^Golia E, Limongelli G, Natale F, Fimiani F, Maddaloni V, Pariggiano I, Bianchi R, Crisci M, D'Acierno L, Giordano R, Di Palma G, Conte M, Golino P, Russo MG, Calabrò R, Calabrò PInflammation and cardiovascular disease: from pathogenesis to therapeutic targetCurr Atheroscler Rep.(2014 Sep)
- ^Bertrand MJ, Tardif JCInflammation and beyond: new directions and emerging drugs for treating atherosclerosisExpert Opin Emerg Drugs.(2017 Mar)
- ^Fritsche KLThe science of fatty acids and inflammationAdv Nutr.(2015 May 15)
- ^Rietschel ET, Kirikae T, Schade FU, Mamat U, Schmidt G, Loppnow H, Ulmer AJ, Zähringer U, Seydel U, Di Padova FBacterial endotoxin: molecular relationships of structure to activity and functionFASEB J.(1994 Feb)
- ^Miller SI, Ernst RK, Bader MWLPS, TLR4 and infectious disease diversityNat Rev Microbiol.(2005 Jan)
- ^Copeland S, Warren HS, Lowry SF, Calvano SE, Remick D, Inflammation and the Host Response to Injury InvestigatorsAcute inflammatory response to endotoxin in mice and humansClin Diagn Lab Immunol.(2005 Jan)
- ^Santos S, Oliveira A, Lopes CSystematic review of saturated fatty acids on inflammation and circulating levels of adipokinesNutr Res.(2013 Sep)
- ^Kratz M, Cullen P, Kannenberg F, Kassner A, Fobker M, Abuja PM, Assmann G, Wahrburg UEffects of dietary fatty acids on the composition and oxidizability of low-density lipoproteinEur J Clin Nutr.(2002 Jan)
- ^Chowdhury R, Warnakula S, Kunutsor S, Crowe F, Ward HA, Johnson L, Franco OH, Butterworth AS, Forouhi NG, Thompson SG, Khaw KT, Mozaffarian D, Danesh J, Di Angelantonio EAssociation of dietary, circulating, and supplement fatty acids with coronary risk: a systematic review and meta-analysisAnn Intern Med.(2014 Mar 18)
- ^Siri-Tarino PW, Sun Q, Hu FB, Krauss RMMeta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular diseaseAm J Clin Nutr.(2010 Mar)
- ^Mozaffarian D, Micha R, Wallace SEffects on coronary heart disease of increasing polyunsaturated fat in place of saturated fat: a systematic review and meta-analysis of randomized controlled trialsPLoS Med.(2010 Mar 23)
- ^Ramsden CE, Hibbeln JR, Majchrzak SF, Davis JMn-6 fatty acid-specific and mixed polyunsaturate dietary interventions have different effects on CHD risk: a meta-analysis of randomised controlled trialsBr J Nutr.(2010 Dec)
- ^Hamley SThe effect of replacing saturated fat with mostly n-6 polyunsaturated fat on coronary heart disease: a meta-analysis of randomised controlled trialsNutr J.(2017 May 19)
- ^Månsson HLFatty acids in bovine milk fatFood Nutr Res.(2008)
- ^Huth PJ, Park KMInfluence of dairy product and milk fat consumption on cardiovascular disease risk: a review of the evidenceAdv Nutr.(2012 May 1)
- ^Lovegrove JA, Hobbs DANew perspectives on dairy and cardiovascular healthProc Nutr Soc.(2016 Aug)
- ^Rosqvist F, Smedman A, Lindmark-Månsson H, Paulsson M, Petrus P, Straniero S, Rudling M, Dahlman I, Risérus UPotential role of milk fat globule membrane in modulating plasma lipoproteins, gene expression, and cholesterol metabolism in humans: a randomized studyAm J Clin Nutr.(2015 Jul)
- ^O'Sullivan TA, Hafekost K, Mitrou F, Lawrence DFood sources of saturated fat and the association with mortality: a meta-analysisAm J Public Health.(2013 Sep)
- ^Vlassara H, Cai W, Tripp E, Pyzik R, Yee K, Goldberg L, Tansman L, Chen X, Mani V, Fayad ZA, Nadkarni GN, Striker GE, He JC, Uribarri JOral AGE restriction ameliorates insulin resistance in obese individuals with the metabolic syndrome: a randomised controlled trialDiabetologia.(2016 Oct)
- ^Briggs MA, Petersen KS, Kris-Etherton PMSaturated Fatty Acids and Cardiovascular Disease: Replacements for Saturated Fat to Reduce Cardiovascular RiskHealthcare (Basel).(2017 Jun 21)
- ^Zong G, Li Y, Sampson L, Dougherty LW, Willett WC, Wanders AJ, Alssema M, Zock PL, Hu FB, Sun QMonounsaturated fats from plant and animal sources in relation to risk of coronary heart disease among US men and womenThe American Journal of Clinical Nutrition.(2018)
- ^Hussain G, Schmitt F, Loeffler JP, Gonzalez de Aguilar JLFatting the brain: a brief of recent researchFront Cell Neurosci.(2013 Sep 9)
- ^Fernandes MF, Mutch DM, Leri FThe Relationship between Fatty Acids and Different Depression-Related Brain Regions, and Their Potential Role as Biomarkers of Response to AntidepressantsNutrients.(2017 Mar 17)
- ^Kien CL, Bunn JY, Tompkins CL, Dumas JA, Crain KI, Ebenstein DB, Koves TR, Muoio DMSubstituting dietary monounsaturated fat for saturated fat is associated with increased daily physical activity and resting energy expenditure and with changes in moodAm J Clin Nutr.(2013 Apr)
- ^Dumas JA, Bunn JY, Nickerson J, Crain KI, Ebenstein DB, Tarleton EK, Makarewicz J, Poynter ME, Kien CLDietary saturated fat and monounsaturated fat have reversible effects on brain function and the secretion of pro-inflammatory cytokines in young womenMetabolism.(2016 Oct)
- ^Sartorius T, Ketterer C, Kullmann S, Balzer M, Rotermund C, Binder S, Hallschmid M, Machann J, Schick F, Somoza V, Preissl H, Fritsche A, Häring HU, Hennige AMMonounsaturated fatty acids prevent the aversive effects of obesity on locomotion, brain activity, and sleep behaviorDiabetes.(2012 Jul)
- ^Kaviani S, Cooper JAAppetite responses to high-fat meals or diets of varying fatty acid composition: a comprehensive reviewEur J Clin Nutr.(2017 Oct)
- ^Krishnan S, Cooper JAEffect of dietary fatty acid composition on substrate utilization and body weight maintenance in humansEur J Nutr.(2014 Apr)
- ^Jones PJ, Pencharz PB, Clandinin MTWhole body oxidation of dietary fatty acids: implications for energy utilizationAm J Clin Nutr.(1985 Nov)
- ^Schmidt DE, Allred JB, Kien CLFractional oxidation of chylomicron-derived oleate is greater than that of palmitate in healthy adults fed frequent small mealsJ Lipid Res.(1999 Dec)
- ^Dorgan JF, Judd JT, Longcope C, Brown C, Schatzkin A, Clevidence BA, Campbell WS, Nair PP, Franz C, Kahle L, Taylor PREffects of dietary fat and fiber on plasma and urine androgens and estrogens in men: a controlled feeding studyAm J Clin Nutr.(1996 Dec)
- ^Wang C, Catlin DH, Starcevic B, Heber D, Ambler C, Berman N, Lucas G, Leung A, Schramm K, Lee PW, Hull L, Swerdloff RSLow-fat high-fiber diet decreased serum and urine androgens in menJ Clin Endocrinol Metab.(2005 Jun)
- ^Hämäläinen E, Adlercreutz H, Puska P, Pietinen PDiet and serum sex hormones in healthy menJ Steroid Biochem.(1984 Jan)
- ^Raben A, Kiens B, Richter EA, Rasmussen LB, Svenstrup B, Micic S, Bennett PSerum sex hormones and endurance performance after a lacto-ovo vegetarian and a mixed dietMed Sci Sports Exerc.(1992 Nov)