
Study under review: Energy Drinks Induce Acute Cardiovascular and Metabolic Changes Pointing to Potential Risks for Young Adults: A Randomized Controlled Trial.
If you want to stay on top of the latest nutrition research, check out the Nutrition Examination Research Digest.
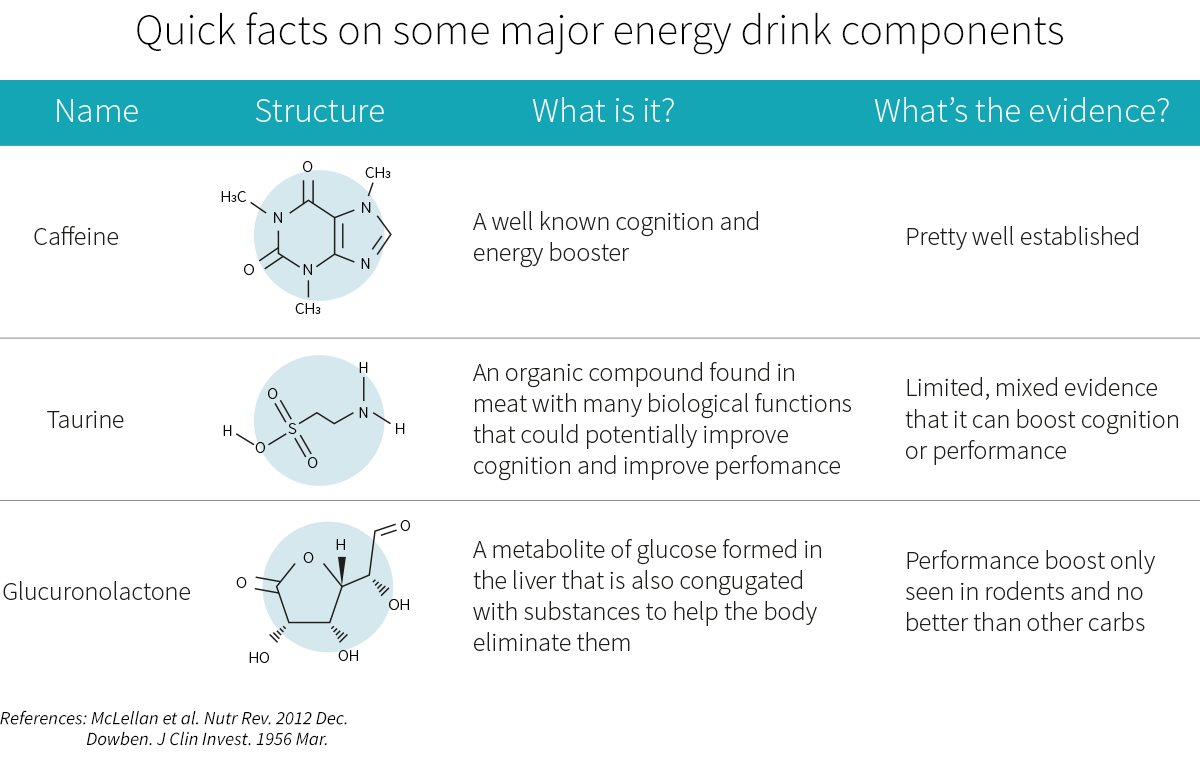
Energy drinks (EDs)[1] are marketed as ‘functional beverages’ and consist of a soda-like drink with high doses of sugar and stimulants to provide a purported energy boost (i.e., it “gives you wings”—although there are no reports of actual wing or feather growth to date). Some of the most common ED ingredients are: caffeine, taurine, glucuronolactone, guarana, ginseng, vitamin B complex, and others. Many of these compounds have not been well studied and are present in EDs at higher doses than recommended[2], yet EDs are reported to be the fastest growing[3] part of the beverage industry.
The primary consumers of these EDs are young men[4] (18-30 years old). Consumption frequency is reported at about one to three days per month[5] in amounts of about one to three liters in a day on average in a German population[6], and an average of 3.1 liters[7] per month in the UK. Commonly reported reasons for use[8] are staying awake, boosting athletic or academic performance, and mixing with alcohol. Most users cannot define ED ingredients and are unaware of the potential adverse effects.
Beyond rare cases of arrest[9] following overconsumption of EDs, common reported adverse effects[10] include cardiovascular (e.g. tachycardia—rapid heart rate, high blood pressure (BP)), gastrointestinal, and neurological (e.g. anxiety, irritability) changes. Moreover, caffeine[11] is one of the only ED ingredients with documented adverse potential, while other common ED ingredients have not been well researched. It is not clear which components or combination of ingredients in EDs contribute to the adverse effects, or whether higher doses may lead to greater adverse effects than lower doses.
The authors of the study under review aimed to examine cardiovascular and metabolic effects of EDs and their major active ingredients (caffeine, taurine, glucuronolactone, or caffeine plus taurine) to determine whether one component or a combination of them is to blame for the reported adverse effects. The putative effects of these components are laid out in Figure 1.
With their high sugar and stimulant content, energy drinks are marketed to young adults who tend to use them to stay awake, boost athletic performance, and mix with alcohol. Beyond rare cases of cardiac arrest, common reported adverse effects include cardiovascular, gastrointestinal, and neurological disturbances, but the specific ingredient or combinations of ingredients that cause these adverse effects is unknown. The study under review aimed to determine the nature of any dose-dependent influence on adverse effects and attempts to distinguish which ingredient(-combination) might be causing these effects.
Who and what was studied?
This was a preregistered[12] randomized, double-blind, crossover trial of 38 young adults (aged 18-25 years) that evaluated the influence of EDs and ED ingredients on cardiovascular and metabolic health. The participants had to be healthy and of normal weight, not regularly consuming coffee (less than one cup per day), alcohol (less than 2 drinks per week for women and 4 for men), or energy drinks (less than 500 milliliters per week). The participants were also all leisurely active; none were athletes, but they weren’t completely sedentary either.
The study design is illustrated in Figure 2. After being matched for sex and smoking status, the participants were randomized into two groups that consumed either 750 milliliters or 1,000 milliliters of a control electrolyte beverage (CP), CP plus 400 milligrams of taurine per 100 milliliters (CP+T), CP plus 32 milligrams of caffeine per 100 milliliters (CP+C), or a Red Bull energy drink (ED). Testing was performed for 11 hours after consuming each beverage, and there were at least four days of washout between tests.
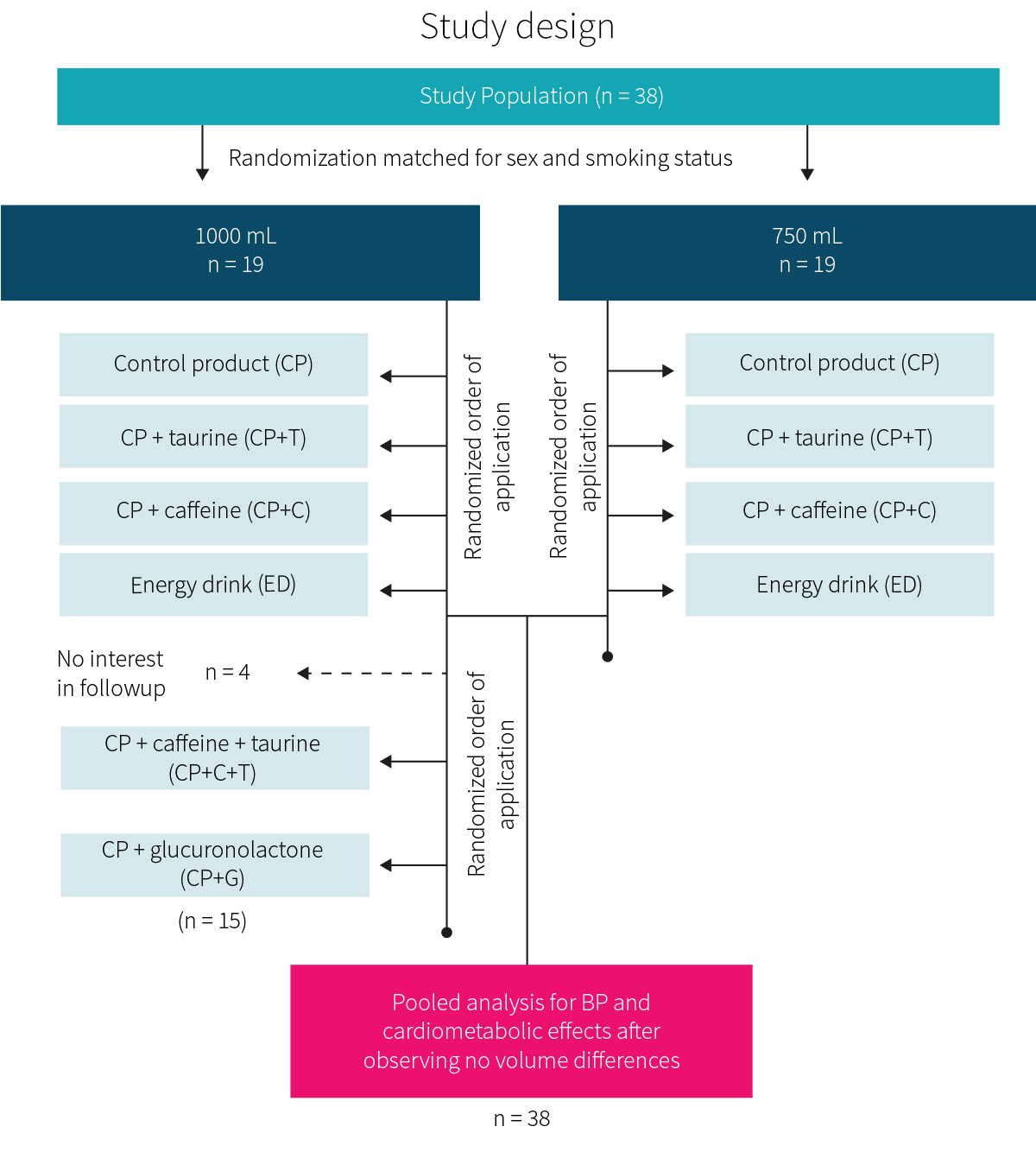
A subset of individuals from the 1,000 milliliter group also consumed two additional test beverages: CP + caffeine + taurine (CP+C+T) and CP + 31 milligrams of glucuronolactone per 100 milliliters (CP+G), also in a randomized crossover design.
Tests were performed in the morning in a fasted state. Blood pressure, electrocardiography (ECG), and subjective symptoms were assessed at baseline and one, three, seven, and 11 hours after consuming the test beverages. Blood samples were collected at baseline and one hour post-beverage.
The only outcome listed in the preregistration was the primary outcome of heart rate variability (HRV). In the study manuscript, blood pressure was stated to be the primary outcome, with all other cardiovascular variables (mean arterial pressure (MAP = (⅓) systolic BP + (⅔) diastolic BP; a measure of the average pressure arteries are under, which is a function of both cardiac output and resistance of blood vessels), QTc interval, and heart rate) being secondary outcomes alongside all bloodborne measurements (glucose, insulin, electrolytes, and caffeine) and a symptoms questionnaire.
This randomized, double-blind, crossover trial in 38 young, leisurely active adults (aged 18-25 years) evaluated the influence of EDs and ED ingredients on cardiovascular and metabolic health. The primary outcome was blood pressure, while secondary measures were mean arterial pressure, QTc interval, heart rate, and serum metabolic markers.
What were the findings?
As expected due to the different caffeine concentrations, the 1,000 milliliter CP+C and ED groups experienced greater rises in serum caffeine concentrations than the 750 milliliter groups. There were no other differences in any outcome between the two different beverage sizes, so data was combined when possible.
During the first hour after consumption, all caffeine-containing beverages (CP+C, CP+C+T, and ED) significantly increased diastolic blood pressure, while the ED and CP+C beverages also increased systolic blood pressure. Changes were modest, however, amounting to no more than about eight mmHg systolic and five mmHg diastolic, and returned to baseline during the three-hour check.
During the first hour after consumption, MAP was increased in the ED, CP+C groups, and CP+C+T groups only, by about three to seven mmHg. Heart rate was slightly elevated in the ED group by four beats per minute. The QTc interval was shortened in the CP+C+T and CP+G groups.
Every beverage, including the control, increased insulin and reduced glucose, albeit less significantly than insulin, resulting in an increase in HOMA-IR. The effects were greatest with the ED, then the CP+C, while all others were similar in magnitude. However, there was substantial individual variability, with many outliers within each group.
Finally, a marginal increase of reported adverse symptoms occurred following ED intake, but no statistical significance was reached. Five out of 38 participants reported severe symptoms (severe nausea, severe tremor, and severe restlessness) upon administration of ED or CP + C. No cardiac arrhythmias were observed.
Other than expected serum caffeine effects, no differences in any outcome were noted between beverages of differing size. Most effects were observed with beverages containing caffeine, suggesting that it is the primary active ingredient in energy drinks causing cardiovascular and metabolic effects. Serious adverse cardiovascular effects were not observed.
What does the study really tell us?
This study suggests that ED consumption can cause minor, possibly adverse changes in BP, HR, QTc intervals, and glucose metabolism in young and healthy individuals. No arrhythmias or other serious problems were observed, though.
Whether these changes of a couple beats per minute or mmHg of blood pressure are clinically significant regarding increased cardiovascular risk or adverse outcomes in the long run is not clear. In the short term, these adverse effects are likely too small to lead to clinical consequences in generally healthy young adults — although it could precipitate a heart attack in someone who’s already on the verge of having one. And of course, the poison is in the dose: one liter was used in this study, and while some populations might consume one to three liters in one day, most likely aren’t consuming a liter in one hour. A survey[18] from the U.S. suggests that about half of college students drink at least one drink per month, but less than a quarter drink two or more.
Although the analysis of ED components suggest that caffeine may be a driving factor for ED’s adverse effects because of its impact on MAP, the other cardiovascular and metabolic effects cannot be clearly attributed to common single components of EDs tested in this study (caffeine, taurine, or glucuronolactone) because, although the ED-ingredients were isolated, the differences between beverages with only one ED ingredient were not significant enough.
The study was well designed and controlled for the goal of the study. The CP was relatively similar to the ED, without the common ED components of interest, allowing for a well controlled setup to evaluate the influence of each singular common ED component.
Nonetheless, there were several limitations of this study. Beverages were consumed on an empty stomach, potentially causing stronger effects of the ED components being monitored. The sample size was quite small, even after pooling all the data, and although the study population represents the main consumers of EDs, it should be said that healthy young adults are likely less prone to adverse effects in comparison to older individuals that might already have cardiovascular complications. Hence, it is possible that these changes could negatively impact older or more sickly individuals, but this study cannot definitively show this.
Probably most important to keep in mind, though, is that the observations were only short term, following one dosage of the beverage. Although it seems the effects of EDs are relatively short-lived, some components such as caffeine and taurine may have an impact lasting longer than 11 hours. Moreover, this study does not rule out any ED effects that could accumulate following daily consumption and aggravate the seemingly mild adverse effects.
In this context, it’s also worth pointing out a problem with the authors’ use of the measure for insulin metabolism (HOMA-IR). This was originally developed[19] as a quick and easy way to approximate results from the gold standard hyperinsulinemic-euglycemic clamp technique for measuring insulin resistance, and normally uses fasting measures of insulin and glucose to accomplish this. However, they used this equation to measure insulin resistance by looking at insulin and glucose changes one hour after imbibing the ED, which is not how the equation really works. Because of this, interpreting the changes in HOMA-IR that the authors calculated as real changes in insulin resistance should be done with a large amount of caution; it’s quite possible that there was no impact on actual insulin resistance over this short time span.
ED consumption can cause possibly adverse changes in BP, HR, QTc intervals, and glucose metabolism in young and healthy individuals, but whether these changes are potent enough to actually harm the average young and healthy consumer is unlikely. The only single ED component with some individual impact on cardiovascular outcomes (increased MAP) was caffeine. Although the study was well designed and controlled, the observations were only short term, following a single dosage on an empty stomach and thus do not allow for the prediction of cumulative long-term effects. Moreover, the focus on young healthy individuals limits the applicability of the results in potentially higher risk populations, such as elderly individuals or people with pre-existing cardiovascular disease.
The big picture
Previous research has demonstrated adverse effects of EDs on cardiovascular measures. One RCT[20] demonstrated elevations of both systolic and diastolic BP along with increased HR and cardiac output in 25 young healthy adults following consumption of 355 milliliters of an ED. Another RCT[21] demonstrated elevations in BP, but no increase in HR, in 25 young healthy males following consumption of 480 milliliters of an ED. Contrary to these studies, one double-blind trial[22] did not demonstrate any effect on cardiovascular function or blood glucose levels following consumption of 250 milliliters of an ED in 68 healthy adults. The study under review demonstrated changes is in conflict with some of these results, but as the doses of EDs administered were higher (750 milliliters and 1,000 milliliters)—a direct 1:1 comparison is of very limited significance.
A previous review[23] suggests that caffeine induces an impaired glucose tolerance as whole body glucose disposal was reduced by about 30% with caffeine intake. The study under review shares similar findings, demonstrating changes in glucose metabolism following ED consumption, a reduction in insulin sensitivity following ED consumption, but whether this is attributed to the caffeine content alone is not certain. The high sugar in the EDs is obviously a red flag[24] for metabolic diseases, but this relationship has to do with dosages and balance rather than the ingredients in question.
The sheer amount of caffeine in the EDs has been suggested as the cause for adverse cardiovascular effects following ED consumption, with 85% of U.S. parents[25] favoring regulations for caffeine warning labels on energy drinks. With levels of caffeine in EDs ranging from 50-500 milligrams and an average intake of 390 milliliters of EDs according to a systematic review[26], this still shouldn’t be too much of a cause for concern. Caffeine only becomes toxic at levels of about 15 milligrams per kilogram of bodyweight[27], which for a 150 pound (68 kilogram) individual means one gram will be toxic and about 10 grams will be lethal. In the study under review, even at one liter of ED intake, the caffeine content was 320 milligrams, which is equivalent to about two cups of brewed coffee, and below the 400 milligram per day suggested safe upper limit. Whether there is a genetic variant of the caffeine metabolism (CYP1A2) that predisposes individuals to a greater risk[28] of cardiovascular events is unclear given conflicting evidence[29].
While the changes in cardiovascular measures demonstrated in the study under review are possibly too small to trigger short-term clinical consequences in healthy individuals, the settings or circumstances in which they are generally consumed[3] (late night studying, athletics, night clubs), and what they may be mixed[30] with (alcohol, drugs) raise concern and may induce just enough disruption in a healthy individual for clinically relevant side effects (such as the rare cases of cardiac arrest) to occur.
Research regarding the influence of energy drinks on cardiovascular measures is inconclusive—possibly due to dosage and/or ingredient differences of the test beverage. The same goes for changes in glucose metabolism. While excess caffeine intake might be a driving factor behind the adverse effects, this is also not certain and may or may not depend on genetics. The adverse effects are likely not large enough to trigger short-term clinical consequences in healthy individuals, but the small changes may raise concern if combined with other adverse events, actions, or circumstances, and cumulative long-term effects have not been studied.
Frequently asked questions
Q. Why is the combination of energy drinks and alcohol so popular and dangerous?
In 2017, over 10 % of students in grades 8, 10, and 12 and over 30% of young adults (19-28 years old) consumed alcohol mixed with an energy drink[31] at least once in a year. Binge drinkers are also more than twice as likely to mix alcohol with energy drinks. Given the stimulatory effect of energy drinks, when in concert with alcohol, the consumer feels much more alert than they would after the same amount of alcoholic drinks, so they may continue to drink more and increase their risk[32] of drunk driving, unwanted or unprotected sex, or sustaining alcohol-related injuries.
Q. What are energy drinks good for?
The International Society of Sports Nutrition’s position statement on energy drinks[33] suggests that the main ergogenic (athletic enhancing) ingredients are caffeine and sugar—the former provides mental focus, alertness, and improves performance while the latter provides quick energy. A review[18] confirms this position, along with presenting some evidence for improvements in cognitive performance, but suggests there are more adverse effects (metabolic, dental, sleep, stress, and more) that might outweigh the positives.
What should I know?
This randomized, double-blind, crossover controlled trial of 38 young adults (aged 18-25 years) evaluated the influence of energy drinks (EDs) and ED-ingredients on cardiovascular and metabolic health in comparison to a control. Only the ED had an influence on all cardiovascular and metabolic (serum glucose and insulin) measures, while of the tested ingredients, caffeine was the only single ingredient with significant changes in cardiovascular measures.
Other studies demonstrate conflicting results for both cardiovascular health and glucose metabolism. While caffeine is likely a driving factor for part of the cardiovascular adverse effects, and the adverse effects are very small and unlikely to affect young healthy individuals in the short term, the small changes could be a cause for concern if in combination with other substances, activities, and circumstances that increase risk. Future studies should assess the accumulation of long-term effects and related health hazards.
Curious about what the latest research actually says?
If you want to stay on top of the latest nutrition research, check out the Nutrition Examination Research Digest.
Every month, our research team breaks down the most interesting nutrition studies, in exquisite depth and from every angle, using understandable language and helpful infographics.
If you’re a health professional (or you're just a nutrition nerd at heart), the Nutrition Examination Research Digest will pique your curiosity, and save you time and money.
References
- ^Ali F, Rehman H, Babayan Z, Stapleton D, Joshi DDEnergy drinks and their adverse health effects: A systematic review of the current evidencePostgrad Med.(2015 Apr)
- ^Tanne JHNew York attorney general investigates energy drink makersBMJ.(2012 Sep 11)
- ^Energy Drinks: An Assessment of Their Market Size, Consumer Demographics, Ingredient Profile, Functionality, and Regulations in the United States
- ^Bailey RL, Saldanha LG, Dwyer JTEstimating caffeine intake from energy drinks and dietary supplements in the United StatesNutr Rev.(2014 Oct)
- ^Miller KEWired: energy drinks, jock identity, masculine norms, and risk takingJ Am Coll Health.(2008 Mar-Apr)
- ^Event-Related Survey of High Consumers of Energy Drinks
- ^Gathering consumption data on specific consumer groups of energy drinks
- ^Attila S, Çakir BEnergy-drink consumption in college students and associated factorsNutrition.(2011 Mar)
- ^Berger AJ, Alford KCardiac arrest in a young man following excess consumption of caffeinated "energy drinks"Med J Aust.(2009 Jan 5)
- ^Goldfarb M, Tellier C, Thanassoulis GReview of published cases of adverse cardiovascular events after ingestion of energy drinksAm J Cardiol.(2014 Jan 1)
- ^Gunja N, Brown JAEnergy drinks: health risks and toxicityMed J Aust.(2012 Jan 16)
- ^Clinical Trial on the Effects of Caffeine and Taurine From Energy Drinks (EDs) to Parameters of the Cardiovascular System in Humans
- ^Al-Khatib SM, LaPointe NM, Kramer JM, Califf RMWhat clinicians should know about the QT intervalJAMA.(2003 Apr 23-30)
- ^Goldenberg I, Moss AJ, Zareba WQT interval: how to measure it and what is "normal"J Cardiovasc Electrophysiol.(2006 Mar)
- ^Heemskerk CPM, Pereboom M, van Stralen K, Berger FA, van den Bemt PMLA, Kuijper AFM, van der Hoeven RTM, Mantel-Teeuwisse AK, Becker MLRisk factors for QTc interval prolongationEur J Clin Pharmacol.(2018 Feb)
- ^Long QT Syndrome
- ^Short QT syndrome
- ^Malinauskas BM, Aeby VG, Overton RF, Carpenter-Aeby T, Barber-Heidal KA survey of energy drink consumption patterns among college studentsNutr J.(2007 Oct 31)
- ^Wallace TM, Levy JC, Matthews DRUse and abuse of HOMA modelingDiabetes Care.(2004 Jun)
- ^Grasser EK, Yepuri G, Dulloo AG, Montani JPCardio- and cerebrovascular responses to the energy drink Red Bull in young adults: a randomized cross-over studyEur J Nutr.(2014 Oct)
- ^Svatikova A, Covassin N, Somers KR, Somers KV, Soucek F, Kara T, Bukartyk JA Randomized Trial of Cardiovascular Responses to Energy Drink Consumption in Healthy AdultsJAMA.(2015 Nov 17)
- ^Ragsdale FR, Gronli TD, Batool N, Haight N, Mehaffey A, McMahon EC, Nalli TW, Mannello CM, Sell CJ, McCann PJ, Kastello GM, Hooks T, Wilson TEffect of Red Bull energy drink on cardiovascular and renal functionAmino Acids.(2010 Apr)
- ^Shearer J, Graham TEPerformance effects and metabolic consequences of caffeine and caffeinated energy drink consumption on glucose disposalNutr Rev.(2014 Oct)
- ^Loh DA, Moy FM, Zaharan NL, Jalaludin MY, Mohamed ZSugar-sweetened beverage intake and its associations with cardiometabolic risks among adolescentsPediatr Obes.(2017 Feb)
- ^Pomeranz JL, Munsell CR, Harris JLEnergy drinks: an emerging public health hazard for youthJ Public Health Policy.(2013 May)
- ^Burrows T, Pursey K, Neve M, Stanwell PWhat are the health implications associated with the consumption of energy drinks? A systematic reviewNutr Rev.(2013 Mar)
- ^Temple JL, Bernard C, Lipshultz SE, Czachor JD, Westphal JA, Mestre MAThe Safety of Ingested Caffeine: A Comprehensive ReviewFront Psychiatry.(2017 May 26)
- ^Cornelis MC, El-Sohemy A, Kabagambe EK, Campos HCoffee, CYP1A2 genotype, and risk of myocardial infarctionJAMA.(2006 Mar 8)
- ^Zhou A, Hyppönen ELong-term coffee consumption, caffeine metabolism genetics, and risk of cardiovascular disease: a prospective analysis of up to 347,077 individuals and 8368 casesAm J Clin Nutr.(2019 Mar 1)
- ^An assessment of their market size, consumer demographics, ingredient profile, functionality, and regulations in the United States
- ^Fact Sheets - Alcohol and Caffeine
- ^Roemer A, Stockwell TAlcohol Mixed With Energy Drinks and Risk of Injury: A Systematic ReviewJ Stud Alcohol Drugs.(2017 Mar)
- ^Campbell B, Wilborn C, La Bounty P, Taylor L, Nelson MT, Greenwood M, Ziegenfuss TN, Lopez HL, Hoffman JR, Stout JR, Schmitz S, Collins R, Kalman DS, Antonio J, Kreider RBInternational Society of Sports Nutrition position stand: energy drinksJ Int Soc Sports Nutr.(2013 Jan 3)